‘Huge congratulations to Asiya Fatima, runner up of the BSGCT Scientific Writing competition 2026 describing ‘Why timing…

BSGCT Scientific Writing Competition – Runner up – Francisca Wetimane
‘Huge congratulations to Francisa Wetimane, runner up of the BSGCT Scientific Writing competition 2026 describing ‘Rewriting the Code of Life: How Gene Editing is Curing Sickle Cell Disease’.
Francisca Wetimane – Rewriting the Code of Life: How Gene Editing is Curing Sickle Cell Disease
Francisca WETIMANE is a Data Science student at IUT Besançon Vesoul Antenne Dole in France, with a particular interest in applying data-driven approaches to biological and medical research. Drawn to the intersection of technology and life sciences, Francisca combines analytical thinking with a passion for understanding how cutting-edge science can solve real-world health challenges. Their runners-up entry, Rewriting the Code of Life: How Gene Editing is Curing Sickle Cell Disease, reflects this curiosity exploring how CRISPR-based therapy is revolutionising treatment for inherited blood disorders and what it means for the future of genetic medicine. Francisca is a member of the BSGCT student community.”
Rewriting the Code of Life:
How Gene Editing is Curing Sickle Cell Disease
For decades, children born with sickle cell disease faced a lifetime of excruciating pain, frequent hospital visits, and a dramatically shortened lifespan. But in 2023, regulators approved the first CRISPR-based gene therapy for this inherited blood disorder—marking a watershed moment in medicine. For the first time, doctors could permanently correct the genetic mutation responsible for a disease by editing a patient’s own DNA. This breakthrough represents not just a new treatment, but a fundamental shift in how we approach genetic disease.
The Genetic Error Behind Sickle Cell Disease
Sickle cell disease affects millions worldwide, particularly those of African, Mediterranean, and Middle Eastern descent. The condition stems from a single-letter typo in the genetic instruction manual—a mutation in the gene that produces haemoglobin, the protein that carries oxygen in red blood cells[1].
In healthy individuals, red blood cells are round and flexible, allowing them to flow smoothly through blood vessels. However, the mutated haemoglobin in sickle cell patients causes red blood cells to contort into rigid, crescent or ‘sickle’ shapes. These distorted cells become stuck in small blood vessels, blocking blood flow and causing severe pain, organ damage, and strokes. Patients often require regular blood transfusions and pain management, yet until recently, the only potential cure was a bone marrow transplant—a risky procedure requiring a matched donor that fewer than 20% of patients could access[2].
Enter CRISPR: Molecular Scissors for DNA
CRISPR-Cas9, often simply called CRISPR, is a revolutionary gene-editing tool adapted from a bacterial immune system. Think of it as a programmable pair of molecular scissors that can locate a specific sequence in the three billion letters of human DNA, cut it precisely, and allow scientists to make targeted changes. The acronym stands for Clustered Regularly Interspaced Short Palindromic Repeats—referring to the DNA sequences bacteria use to ‘remember’ and fight off viruses[3].
Unlike previous gene therapy approaches that added new genes, CRISPR can directly edit existing genetic code. This precision has transformed what’s possible in treating genetic diseases. The technology works through a two-part system: a guide RNA that acts like a GPS coordinate, directing the machinery to the exact location in the genome, and the Cas9 protein, which acts as the scissors to cut the DNA at that specific spot. Once cut, the cell’s natural repair mechanisms can be harnessed to either disable a problematic gene or correct a mutation.
A Cure Built from the Patient’s Own Cells
The approved sickle cell gene therapy, called Casgevy (exa-cel), uses an ingenious approach. Rather than trying to fix the mutated adult haemoglobin gene directly, it instead reactivates a different version of haemoglobin that we all naturally produce before birth—fetal haemoglobin. This fetal version doesn’t cause sickling and could theoretically substitute for the defective adult form.
The treatment process combines cell therapy with gene editing in several steps (see Figure 1):
1. Collection: Stem cells are harvested from the patient’s bone marrow. These are the master cells that produce all blood cells.
2. Editing: In the laboratory, CRISPR is used to make a precise edit in the BCL11A gene. This gene normally switches off fetal haemoglobin production after birth. The CRISPR edit disrupts this switch, allowing fetal haemoglobin to be produced again.
3. Preparation: The patient undergoes chemotherapy to clear space in the bone marrow for the edited cells.
4. Infusion: The edited stem cells are infused back into the patient, where they establish themselves in the bone marrow and begin producing healthy red blood cells rich in fetal haemoglobin[4].
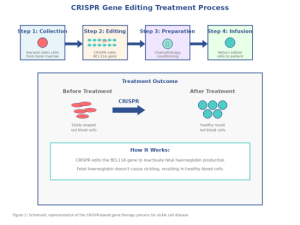
Figure 1: Schematic representation of the CRISPR-based gene therapy process for sickle cell disease.
Transforming Lives: Early Success Stories
The results from clinical trials have been remarkable. Victoria Gray, one of the first patients treated, had experienced severe pain crises nearly every month for most of her life. After receiving the gene-edited cells, she has been essentially symptom-free for over four years. In the pivotal trials, 29 of 31 patients who could be evaluated were free from severe pain crises for at least 12 consecutive months following treatment—a dramatic improvement for a disease that had dominated their entire lives[5].
These aren’t temporary improvements—the edited cells continue producing fetal haemoglobin, creating what appears to be a functional cure. Patients who previously required frequent hospitalisations and blood transfusions are now living normal lives. The therapy offers something no conventional treatment could: a one-time intervention that addresses the root genetic cause of the disease.
Beyond Sickle Cell: A New Era of Genetic Medicine
The approval of CRISPR therapy for sickle cell disease represents far more than a single treatment—it validates gene editing as a viable medical approach and opens doors for treating thousands of other genetic conditions. Similar CRISPR-based therapies are now in clinical trials for beta-thalassemia, certain cancers, inherited blindness, and various metabolic disorders[6].
Challenges remain. The current treatment is complex, expensive (around £2 million per patient), and requires intensive chemotherapy conditioning that carries risks. Scientists are working on next-generation approaches that could make gene editing safer, more accessible, and applicable to more diseases. These include improved delivery methods that could edit cells directly in the body, refined CRISPR tools with enhanced precision, and strategies to reduce the need for harsh chemotherapy.
Yet the fundamental principle has been proven: we can now rewrite the human genetic code to cure disease. As one researcher noted, we’ve moved from reading the book of life to editing it. For patients with sickle cell disease and countless other genetic conditions, this represents not just hope, but a genuine revolution in medicine—one that’s already changing lives.
References
[1] Kato GJ, Piel FB, Reid CD, et al. Sickle cell disease. Nat Rev Dis Primers. 2018;4:18010.
[2] Gluckman E, Cappelli B, Bernaudin F, et al. Sickle cell disease: an international survey of results of HLA-identical sibling hematopoietic stem cell transplantation. Blood. 2017;129(11):1548-1556.
[3] Doudna JA, Charpentier E. The new frontier of genome engineering with CRISPR-Cas9. Science. 2014;346(6213):1258096.
[4] Frangoul H, Altshuler D, Cappellini MD, et al. CRISPR-Cas9 gene editing for sickle cell disease and β-thalassemia. N Engl J Med. 2021;384(3):252-260.
[5] Vertex Pharmaceuticals and CRISPR Therapeutics. CASGEVY (exagamglogene autotemcel): FDA approval summary. 2023.
[6] Uddin F, Rudin CM, Sen T. CRISPR gene therapy: applications, limitations, and implications for the future. Front Oncol. 2020;10:1387.
Related Posts